 Unknown
at
Wednesday, August 10, 2016
Unknown
at
Wednesday, August 10, 2016
I've been consistently told that after each rotation, as in the Hozier song "Someone New," you'll fall in love just a little ol' little bit every day with some new pharmacy practice area [sic].
That happened for me in the Surgical Intensive Care Unit, or SICU, aptly pronounced as it houses the most critically ill patients in the hospital. I had the awesome opportunity of rotating at a newly dubbed Level 1 Trauma Center in a 20-bed unit comprised of patients from the Trauma Critical Care Service (TCCS) and Cardiothoracic Surgery Service (CTS): trauma surgery, cardiothoracic surgery, neurosurgery, vascular surgery, colorectal surgery, general surgery, otolaryngology, obstetrics, and orthopedic surgery.
Surgery isn't covered in our didactic curriculum, so I started the first day as a total derp (Deer in headlights with Extreme anxiety and Retrograde amnesia of Pharmacology). Thankfully, my preceptor reassured me that every P4 student feels the same way at first, and that I'd learn exponentially more on rotation than I ever did in class.
Pro-tip to avoid being a derp at any inpatient rotation: get familiar with your organization's intranet. Like, be best buds with that guy. An intranet is an electronic and readily available Room of Requirement. My personified conversations with the intranet went something like:
"How's the susceptibility to Bactrim here?"
"BOOM."
"Yo, can we get rid of the IV PPI?"
"I got 99 million guidelines and Stress Ulcer Prophylaxis is one."
"Are any of these 14 drugs dialyzable?"
"
 "
"What was a typical day like?
I arrived at 6:30 to work up patients until rounds. Once we had gauged the number and acuity of the patients on the floor that morning, my preceptor and I would round with either TCCS at 9:00 or CTS at 8:45. TCCS is a teaching service that consists of an attending surgical intensivist, surgical critical care fellow, surgical and medical residents, a clinical dietician, a respiratory therapist, nursing, and a clinical pharmacist on rounds, whereas CTS is physician assistant-led. Side note: the health care professionals I worked with are truly impressive. Many of them are nationally renowned in their respective specialties, and the cardiac surgery program here ranks in the top 15 in the nation (among 400+ other hospitals' Consumer Reports' Ratings).
After rounds, which lasted anywhere from an hour to several hours depending on how many patients were on the service, I would often bombard my preceptor with a myriad of questions. Side note: the thing about being curious and wanting to learn is that it'll almost always result in self-assigned drug info questions, which present as both a curse and a blessing in disguise. I encourage you to embrace this curse.

I had 1-2 critical care topic discussions each day with my preceptor before and/or after lunch, which helped keep me on my toes. In the afternoons, I'd re-work up my patients to see what changes were made after rounds and/or any surgeries and give patient presentations to my preceptor.
What neat stuff did you get to see?
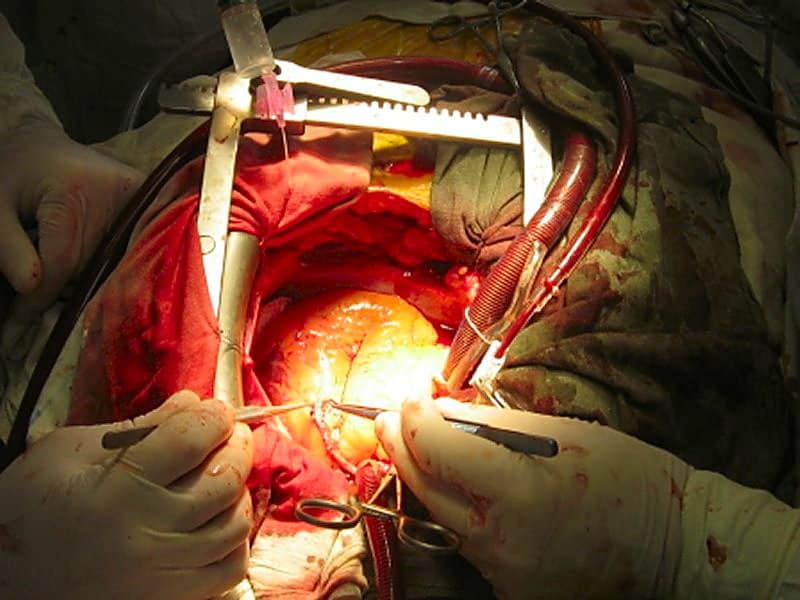
Neutropenic enterocolitis, esophageal rupture, necrotizing pancreatitis, aortic dissection, traumatic brain injury, motor vehicle accidents, buzzword buzzword. Also got a bird's eye view of a coronary artery bypass graft (CABG) and saw a lower lobectomy.
What do you wish you knew going into the rotation? How can I prepare? Clinical pearls? Coffee choice? HALP
I finally realized that having a wealth of education as a P4 student isn't necessarily what leads to success. Initially, I was mortified by my extreme deficit of therapeutic knowledge. But while pharmacists need to know a lot of information, they don't necessarily have to memorize every detail of every drug ever made (just most of them, ha!). Pharmacy school can't teach you everything you need to know in 3 years. What it can do is teach you how to think like a pharmacist and how to find the information you need to facilitate patient care.
Something you don't learn from a textbook is how to interact with the medical team to optimize treatment. I've decided that I need to create some sort of cheesy alliteration to help others combat this, and I hereby give you the three C's:
- Confidence: You can be incredibly informed on a certain subject and still appear as unintelligent if you're visibly nervous. Some of my battles during this rotation were convincing myself that I actually did know what I was doing and beginning to speak up during rounds. Certainly don't rattle off about something you're not 100% sure about—that's what the "I'll look it up and get back to you" card is for. But speak with conviction, and more people will take heed of your recommendations (even if you're a student who's rounding alone!)
- Camaraderie: If you don't get along with the people you work with, team decision-making is going to be as productive as a day in the life of Snorlax. I had the opportunity to talk to PAs, nurses, residents, patients, and their families about things unrelated to work (like Ann Arbor restaurants and mutual desires for caffeine gtts). Walking up to someone, being personable, and making a recommendation face-to-face is much more effective than paging someone in what might be interpreted as a passive-aggressive tone.
- Credibility: You know who you should add to your BFF list along with the intranet? Evidence-based medicine (EBM). EBM is the realest thing you'll use to stay up to date with pharmacy after you've left the classroom. Your recommendations will be more compelling if they're supported by well-designed, peer-reviewed research. Keep up to date with the lit—there's an app for that.
Actually, instead of using cheesy alliteration, you could probably just refer to Aristotle's Modes of Persuasion. (Man, this is like when 14-year-old you thinks you've come up with a catchy guitar riff and it ends up being a Fratellis song because you've listened to Costello Music religiously).
Anyway, these skills really made me feel like a boss as time went on. For example, when a traumatic brain injury patient was newly admitted, I reviewed the patient's profile and discussed 5 interventions I wanted to make with my preceptor before rounds. Sure enough, all of them had been implemented when I checked the medication administration record (MAR) later that day. *mental self-high five*
Any cool pharm perks?
Someone ALWAYS brought in donuts or brownies or chocolate or D) all of the above to share. I'm not a huge sweets person, but the constant supply of glucose I was exposed to was unreal.
I also lunched and learned so hard. Besides the fact that I got free food each Thursday (heyooo), I saw cool presentations about medical decision making for organ donation, ventilator settings and the importance of checking the ABG (arterial blood gas, not aznbbygurl) and M&Ms. M&Ms (Morbidity and Mortality Conferences) are an Accreditation Council for Graduate Medical Education (ACGME) mandated educational series that occur regularly at all institutions that have residency training programs. The medical team reviews real patient cases involving either poor or unintended outcomes which might have been due to or worsened by error, "near misses" in which an error could have resulted in a poor outcome, or interesting and unique cases. Then, they discuss what went wrong, what could have been done differently, and what can be done to prevent such events from occurring in the future. Super sick stuff.
In addition to my day-to-day activities, I wrote antimicrobial stewardship notes, conducted a journal club, and delivered an in-service about the pharmacologic management of pain, agitation, and delirium in the ICU to the CTS team. Overall, this was a great practice site at which clinical pharmacists work alongside and are respected by their colleagues. I'm pretty stoked for my next direct patient care gig. As Hozier says, "Love with every rotation, the stranger the better."
In addition to my day-to-day activities, I wrote antimicrobial stewardship notes, conducted a journal club, and delivered an in-service about the pharmacologic management of pain, agitation, and delirium in the ICU to the CTS team. Overall, this was a great practice site at which clinical pharmacists work alongside and are respected by their colleagues. I'm pretty stoked for my next direct patient care gig. As Hozier says, "Love with every rotation, the stranger the better."

No comments:
Post a Comment